
Typhoid remains a public health threat in many countries, particularly in Southeast Asia and sub-Saharan Africa. Understanding a country’s typhoid burden is often one of the first steps toward prevention and control efforts. Decision-makers need to understand the scale and impact of the typhoid burden to determine how to best allocate limited health sector resources. But typhoid burden often changes over time. Therefore, scale and impact of the disease can be better appreciated using long-term data. My collaborators at KEMRI, CDC, and CDC-Kenya and I recently published a study tracking ten years of typhoid burden in Kibera, a densely populated urban informal settlement in Nairobi, Kenya. Here are three key takeaways from our results.
-
Typhoid is dynamic and incidence can change
Our results showed that typhoid burden is not static and it fluctuates over time. During the early years of the surveillance, typhoid burden was high in Kibera. Between 2010-2012, we saw typhoid rates between 144 to 233 cases per 100,000 people. The World Health Organization classifies high typhoid burden as rates of more than 100 cases per 100,000. Interestingly, between 2013-2018, observed typhoid rates declined substantially. During this period, we found rates between 9 to 55 cases per 100,000.
Many factors could explain the observed changes. The decline in burden may be attributed to improvements in the supply of clean water in the area as part of the Kenyan government’s efforts to provide clean water nationally. It may also have been driven by natural immunity, which may have been acquired during the period of high disease burden when many people were likely exposed. However, the rebound of typhoid burden in 2019, with a rate of 130 cases per 100,000, demonstrates how quickly typhoid risk can emerge without consistent and sustainable prevention measures. This finding highlights the importance of immunization programs with typhoid conjugate vaccines (TCVs) and sustained investment in water, sanitation, and hygiene (WASH) infrastructure improvements for long-term control of typhoid.
-
Children are at highest risk
Throughout the ten years of surveillance data, children 2-9 years old consistently had the highest rates of typhoid. Children 5-9 years old had an incidence rate of 208 cases per 100,000 and children 2-4 years old had an incidence of 173 cases per 100,000. This finding is consistent with many other surveillance studies showing that typhoid burden disproportionately impacts young children.
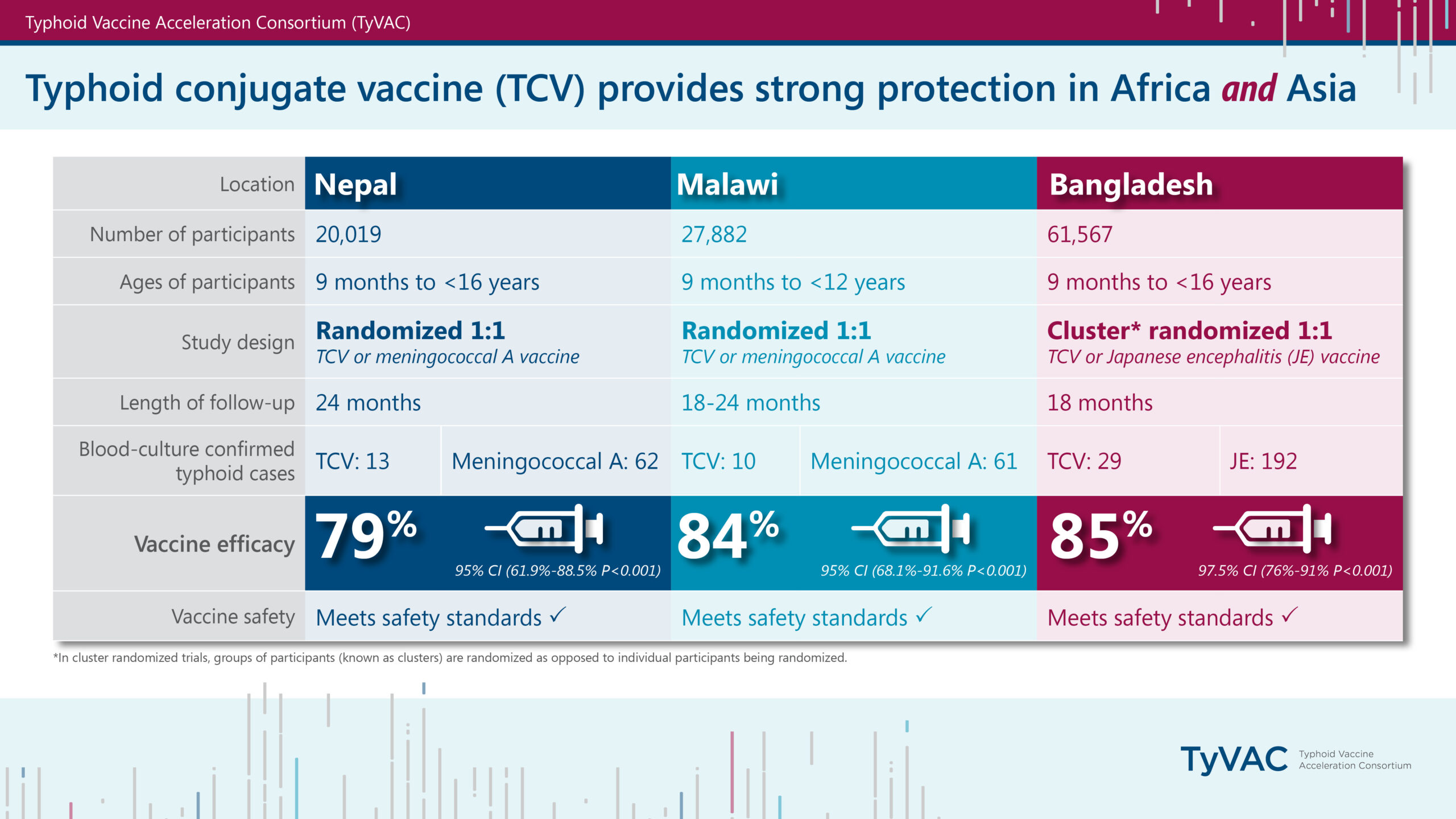
TCVs could have a major impact on reducing typhoid burden in Kibera. TCVs are highly effective and safe for children as young as 6 months old, providing protection to those most at risk for typhoid infections. Data from Malawi show that TCVs are 84% effective among children younger than 15 years old.
-
Drug-resistant typhoid remains a persistent threat and challenge
Multidrug-resistant (MDR) typhoid was consistently identified throughout the study period; 72% of samples were MDR. This means that these strains are resistant to three classes of antibiotics commonly used to treat typhoid. As treatment practices changed over time to respond to resistance trends, we saw an increase in the number of samples with decreased susceptibility to ciprofloxacin, the current standard treatment option in Kenya, beginning in 2013. This means there is an increasing number of drug resistant samples that aren’t responding to this standard antibiotic treatment.
Continued typhoid diagnosis and monitoring of drug-resistance trends in Kibera can help guide treatment practices to ensure that those who do get sick receive appropriate antibiotic treatment. Additionally, TCVs are highly effective against drug-resistant strains. By preventing typhoid infections, we can reduce antimicrobial use and the emergence of drug-resistant infections.
The long-term data provided by this study provide insights for decision-makers to help guide typhoid control strategies. An accompanying editorial also highlights why long-term burden data from a single site are so important for tracking typhoid trends over time. Our findings show a variable but persistently high typhoid burden in Kibera. The latest data from 2019 show an increasing trend. TCVs are a critical tool that can help address the high typhoid burden observed in Kibera, particularly among children. TCV introduction into the childhood vaccination program could substantially reduce the burden in children who are at highest risk. An integrated approach that also includes WASH improvements could have the highest impact on typhoid in Kibera in the long-term.
The Government of Kenya plans to introduce TCV into the routine childhood immunization schedule in 2024. This decision will benefit communities across Kenya, including Kibera, protecting children from typhoid for years to come.
Photo: TyVAC/Madalitso Mvula.

{kind=link}